
The Laparoscopic Adjustable Gastric Band
 The laparoscopic adjustable gastric band (lap band) became an increasingly popular method for weight loss in Australia and Europe in the 1990s. In 2001 the FDA approved the LAP-BAND System for use in the United States. At this time, there are two FDA approved adjustable gastric band systems that are available to patients interested in surgical weight loss in the US. The systems are: LAP-BAND System (Allergan) and The Realize Band (Ethicon).
The laparoscopic adjustable gastric band (lap band) became an increasingly popular method for weight loss in Australia and Europe in the 1990s. In 2001 the FDA approved the LAP-BAND System for use in the United States. At this time, there are two FDA approved adjustable gastric band systems that are available to patients interested in surgical weight loss in the US. The systems are: LAP-BAND System (Allergan) and The Realize Band (Ethicon).
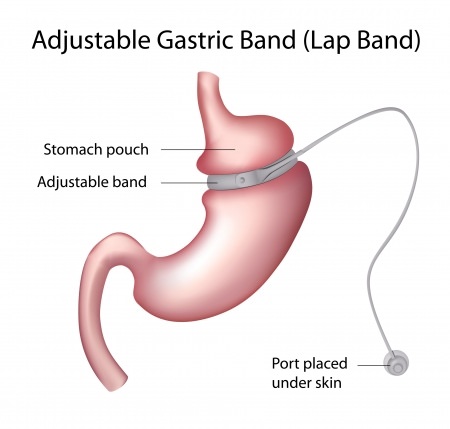
Both devices work in a similar fashion. The laparoscopic adjustable gastric band is placed around the upper portion of the stomach and secured. The band acts by partitioning the stomach into an “upper pouch” and a lower “stomach reservoir”. The device is intended to provide restriction. That is, small amounts of food fill the upper pouch and quickly give the individual a sense of fullness or satiety. The food then passes through the band and into the remainder of the stomach. The rest of digestion and absorption occurs, as it would have prior to placement of the band.
The band is connected to a small port that is anchored to strong connective tissue on top of the muscles of the abdominal wall by means of a thin tube. In the office, the port can be felt underneath the skin and accessed with a small needle. Through the port, saline (sterile salt water) is injected and the fluid is transferred to an empty ring within the lap band. As the band is inflated with fluid, the opening between the small upper pouch and lower stomach becomes smaller. By doing this, food provides a sense of fullness in a shorter period of time and patients experience less hunger.
Weight Loss
There have been many studies that have demonstrated significant weight loss with the LAP-BAND/Realize Band systems. However, at this time, most bariatric surgeons agree that the amount of weight lost, length of time to lose the weight and the predictability of a patient losing significant weight are not the same as those patients who have had either the sleeve gastrectomy or the gastric bypass.
I give my patients an annual weight loss goal of 50 lbs irrespective of their initial weight. This generally equates to a loss of one pound every week. With an intense exercise regimen and following strict dietary guidelines some patients may attain a weight loss of 2 lbs per week.
Prospective patients must also be aware and understand that optimal weight loss requires repeated office visits. At each office visit the doctor and patient will determine whether or not a band adjustment is necessary. The data has demonstrated that patients who adhere to their office visit schedule are much more likely to have success losing weight.
Complications with the Laparoscopic Adjustable Gastric Band
All surgery poses the risk of having a complication. Patients are at risk for complications that aren’t unique to bariatric surgery. Fortunately, the majority of complications that occur are generally not life threatening and can be managed without further surgery. Complications associated with the laparoscopic adjustable gastric band are categorized as “early” and “late” complications. Early complications are generally those that occur right around the time of surgery or within the first 30 days. Late complications generally occur from one month to years after the procedure.
Early complications
Bleeding
Significant blood loss or hemorrhage is an uncommon event. The source of blood loss is usually from the dense network of blood vessels that surround the upper stomach and injury to the spleen during passage of the band around the upper stomach. Although the need for blood transfusion is uncommon it may be necessary as a life saving maneuver. In rare cases an emergency spleenectomy might be required.
Perforation
Injury to the esophagus or stomach while creating a tunnel for passage of the band around the upper stomach can cause a perforation. A perforation can lead to peritonitis, a potentially deadly form of intra-abdominal infection. The risk of having a perforation is extremely low.
Deep Vein Thrombosis/Pulmonary Embolism
DVT (deep vein thrombosis) describes a blood clot that forms within the veins of the pelvis or leg. A DVT can cause leg swelling and pain. A DVT becomes more problematic if the clot dislodges and travels to the heart and is then pumped into the pulmonary (lung) arteries. This is referred to as a PE (pulmonary embolism). A PE can place significant strain on the heart and if left untreated can have major consequences. Treatment requires the use of a blood thinner for a period of 3 months to a full year. In some cases, medical treatment with a blood thinner could be life-long.
Several precautions are taken to reduce the chances of developing a DVT/PE. This includes the use of blood thinners prior to and after surgery. In some patients blood thinners may be necessary even after discharge. In addition, SCD (serial compression device) boots are placed on the patients lower legs prior to surgery and remain in place until the patient is up into a chair and walking.
The risk of developing a DVT depends on a number of factors. Dr Laker will be able to give you an idea of what your risk is based on your history and a number of other factors. Overall, the risk of developing a DVT is quite small, approximately 0.5-2%. Of those patients who develop a DVT the risk of having a PE is also very low.
Wound infection
Infections at the incision sites are uncommon when the procedure is performed in a laparoscopic fashion. However, should your operation need to be converted to an open procedure there is a substantially higher chance of developing a surgical site infection. Post-operative wound infections can generally be treated with local wound care (dressing changes) and potentially a course of antibiotics.
Death
Large studies have demonstrated the potential of dying as a result of complications after laparoscopic adjustable gastric band surgery to be exceptionally low.
Late complications
“slipped band”
“Slips”, also referred to as gastric prolapse, occur when the stomach beneath the band slides underneath the band. This essentially creates an obstruction at the level of the band. Food intolerance and vomiting shortly after eating often accompany a slip. In certain situations a slip can be life threatening if the blood supply to the stomach is compromised. Slips can sometimes be managed by removing fluid from the system. Other times, the problem requires surgery to correct. The surgical literature demonstrates a wide range of the chances of developing a slip from 1 to 15%.
Band erosion
Over a period of time the band can cause tissue breakdown and eventually erode through the wall of the stomach. The band must then be removed.