
Incisional hernia
What is an incisional hernia?
Incisional hernias are defects of the abdominal wall that develop through a previous surgical incision of the abdominal wall. The chances of developing a incisional hernia is related to several factors such as weight, age, over-all health, underlying medical issues, family history, size of the incision and wound issues that may have developed after the initial operation. The surgical literature has demonstrated that the risk of developing in incisional hernia is in the range of 10 to 40% after a mid-line abdominal incision.

How are incisional hernias repaired?
At this time, most surgeons would agree that repairing incisional hernias is best accomplished with using mesh. The type of mesh used is often determined by method of repair, size of the defect, the patient’s body habitus and the manner a patient presents with the problem. The surgical literature has demonstrated clear and convincing evidence that the recurrence rate is significantly lower when incisional hernias are repaired using mesh.
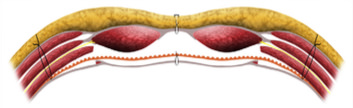
The key to repair is having wide coverage of the defect. This is best accomplished using one of the component separation techniques. The component separation techniques allows for the release of either the anterior or posterior components of the abdominal wall. This provides laxity to the muscles and allows for closure of larger defects. In addition, most component separations are done placing the mesh either behind the entire abdominal wall or beneath the rectus muscles.
The following repairs are performed in an open manner, laparoscopic and robotically. There are times when different modalities are used for the same patient. In some instances the procedure might be performed using all three techniques to allow for the best outcome.
TARR Technique
Currently, the approach that Dr Laker uses for complex hernia repairs is to release the deepest of the three layers of muscle. This enables very large openings to be closed and also allows for exceptionally wide mesh coverage of the abdominal wall behind the rectus and the lateral muscles of the abdominal wall.
When completed the mesh lies entirely outside of the abdominal cavity, sandwiched in between the anterior and posterior fascial layers of the abdominal wall. This has been referred to as a TAR (transversus abdominus release) or rTAR (robotic transversus abdominus relesase) when performed using the robotic platform. This procedure can also be performed laparoscopically but requires exceptional minimally invasive surgical skills.
eTEP Technique
A recently described technique to address ventral hernias (umbilical, epigastric, Spigelian and incisional) is called eTEP (expanded totally extra-peritoneal) and this can be performed both robotically as well as laparoscopic. The eTEP takes advantage of the layered architecture of the abdominal wall. The mesh is placed in between layers of the abdominal wall, thereby, acting as an underlay patch and in direct contact with musculature. The abdominal cavity is not entered and therefore there is no contact between the mesh and the underlying abdominal organs. At the same time, the mesh is in an ideal location for full tissue integration and incorporation. This diminishes the potential for infections, chronic pain and likely recurrence.
In fact, minimally invasive repairs with mesh for incisional hernia have been shown to have a lower recurrence rate, lower risk of mesh related infections and improved cosmetic results. Patients may also return to activity sooner and have less post-operative pain after laparoscopic repair. Over the last decade, the trend in surgery is to manage incisional hernias in a laparoscopic fashion.
Dr Laker had performed many TARs and eTEPs both robotic, laparoscopic and open to correct massive hernias of the abdominal wall.