
 The adrenal glands are mustard colored, small triangular or crescent shaped organs that are located on the upper pole of both kidneys. A layer of fatty tissue separates the adrenal glands from the kidneys. The adrenal gland is considered an endocrine organ in that it secretes substances into the blood stream that have a major impact on physiologic functions. During periods of stress (exercise, starvation, fear) the adrenal glands produce and release a number of hormones that optimize the body to best manage the stressors.
The adrenal glands are mustard colored, small triangular or crescent shaped organs that are located on the upper pole of both kidneys. A layer of fatty tissue separates the adrenal glands from the kidneys. The adrenal gland is considered an endocrine organ in that it secretes substances into the blood stream that have a major impact on physiologic functions. During periods of stress (exercise, starvation, fear) the adrenal glands produce and release a number of hormones that optimize the body to best manage the stressors.
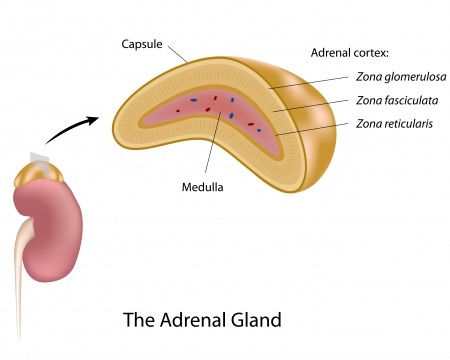
The adrenal gland is composed of two distinct layers: the cortex and the medulla.
 Adrenal Cortex
Adrenal Cortex
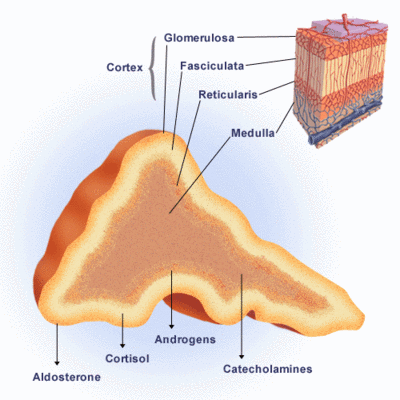
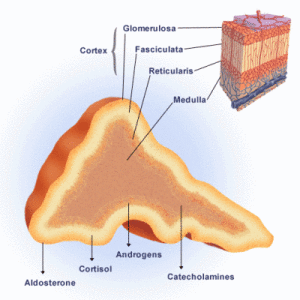
The cortex comprises approximately 80% of the adrenal gland. The cortex is further divided into three separate zones. Each zone produces unique steroid hormones. Steroid hormones are all derived from cholesterol.
Zona glomerulosa:
This is a thin outer layer that is responsible for the production and release of mineralocorticoids, mainly aldosterone. Mineralocorticoids help regulate blood pressure by changing the absorption of electrolytes and water.
Zona fasciculata:
The middle and largest layer of the cortex produces glucocorticoids, commonly referred to as “stress hormones”. Cortisol is the most well-known glucocorticoid hormone. Glucocorticoids effect every organ in a broad variety of ways. The mineralocorticoids raise blood sugar by breaking down lipids, carbohydrates and proteins. Cortisol also has a profound effect on blood pressure, heart function, the immune system, temperature and weight.
Zona reticularis:
The innermost layer produces androgen (male) hormones both in men and women.
Adrenal Medulla
The portion of the gland that is covered by the cortex is the medulla. In this portion of the adrenal gland, catecholamines are produced and released into the blood circulation. Catecholamines are often referred to as “adrenaline”. Epinephrine and norepinephrine (both catecholamines) increase heart rate, blood pressure, dilate the pupils and relax airway muscles to improve air flow. This is the “fight or flight” response to stress.
Adrenal adenomas
Not infrequently, masses in the adrenal glands are identified on imaging studies like CAT scan or MRI. The majority of these lesions are found incidentally and were not the indication for the imaging study. The term “incidentaloma” has been used for several decades when these incidental adrenal masses are encountered. The question has always been: Should something be done? It is well known that larger lesions are more likely to be functioning. This means that the lesion is secreting any of the number of substances produced by the adrenal gland in higher than normal quantities. Also, adrenal cancer, although very rare, is more likely with larger adrenal lesions.
The current recommendations for lesions found incidentally are:
- Detailed evaluation of patient history and symptoms or signs of a functioning adrenal adenoma
- .Biochemical testing of the blood and urine to determine if there are elevated levels of adrenal hormones or their metabolites.
- Although there is some disagreement, lesions larger than 4 cm should be considered for removal of the adrenal gland. Often, surveillance with repeat imaging studies are performed every three to six months. Interval enlargement of the lesion is another indication for surgical adrenalectomy.
Functioning Adrenal Adenomas
Adrenal adenomas are benign masses that may or may not produce excess hormones. There are several syndromes that are attributed to excess secretion of adrenal hormones.
The most common functional adrenal adenomas are:
Aldosteronoma (Conn’s Disease) – A disease produced by excess production of the mineralocorticoid, aldosterone. The disease is characterized by moderate to severe high blood pressure that is resistant to multiple medications. Over time, low serum potassium levels can also be found.
Cushing’s syndrome – A disease produced by excess production of glucocorticoids, especially cortisol. Other conditions can cause elevated cortisol level. Cushing’s syndrome is specific to the adrenal gland being the site for overproduction of cortisol. There is a wide range of physiologic effects and physical findings. Patients often have high blood pressure and elevated blood sugars. Physical features include: muscle loss in the arms and legs, water retention around the face, enlarged fat mass behind the neck, easy bruising, stretch marks on the skin and fatigue.
Diseases of the Adrenal Medulla
Pheochromocytoma – This is a disease of the adrenal medulla whereby excess “adrenaline” hormones are produced. The symptoms can be mild such as moderate high blood pressure. There may be episodic periods of extremely high blood pressure, heart palpitations and profuse sweating. Pheochromocytomas can be found in both adrenal glands and in areas far away from the adrenal glands, referred to as paragangliomas. Approximately 10% of pheochromocytomas are found to harbor cancer.
Evaluation:
There are a number of blood and urine tests that are used to establish the diagnosis of a functioning adenoma. Additional imaging studies or combined imaging with blood sampling may be required to determine whether the left or right adrenal gland is the problem.
Surgical Management of Adrenal Tumors
Surgery is generally indicated for functioning adrenal masses and adrenal cancer. Fortunately, most indications for adrenal surgery is for benign disease. Adrenal surgery has benefited tremendously from the advancement of laparoscopic surgery. A procedure that was once performed through large flank incision that are prone to hernia formation are now routinely performed with 4 to 5 small incisions. The benefits have been remarkable. Often, patients leave the hospital one to two days after surgery.
The size of the adrenal mass plays a role on whether or not the procedure can be performed laparoscopically. Currently, there is no universally excepted size that precludes using a laparoscopic approach and the literature has cases of laparoscopic adrenalectomy of masses approximately 15 cm. Adrenal cancer has classically been performed in an open fashion for fear of “seeding” the surrounding tissue with cancer. At this time, no consensus has been reached in regards to open vs. laparoscopic surgery for adrenal cancer