
Sports Hernia
A “sports hernia” is a difficult diagnosis to make. There are different theories as to what the underlying pathology is and to underscore the confusion there are several names that have been used to describe the condition: Gilmore’s groin, sportsman’s hernia, athletic pubalgia and osteitis pubis. The injury is often seen in young, elite athletes. The sports that have been most commonly linked with these injuries are football, soccer, ice hockey and tennis. In general, sports or activities that require rapid acceleration and deceleration along with quick changes in direction (cutting) can lead to rapid and powerful muscular contractions. When performed repeatedly the consequence can be chronic groin pain.
In general, there are three major processes that can lead to chronic groin pain. Although there may be subtle differences on physical exam they all share one commonality: there is no obvious inguinal hernia (ie. bulge).
Musculotendinous causes
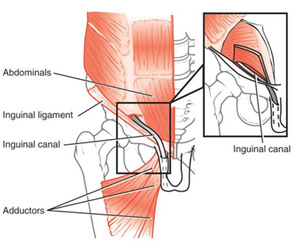 The condition can arise when there is inflammation or avulsion of tendons from the pubic ramus and pubic symphysis. In general, the large muscles of the inner thigh (the adductor muscles) that pull the leg toward the midline generate contractions that tear the connection between the tendon and the pubic bone. This often leads to inflammation and swelling that is perceived as pain in the area when examined and demonstrates specific findings of swelling, muscle separation and boney changes on MRI. The rectus muscle counterbalances the adductor muscles and they too can be torn and injured. This is usually the result of having stronger adductor muscles than rectus muscle. The treatment should first be rest and under the guidance of a physician or therapist NSAIDs may be used. Most individuals will require 3 months of reduced activity and rest.
The condition can arise when there is inflammation or avulsion of tendons from the pubic ramus and pubic symphysis. In general, the large muscles of the inner thigh (the adductor muscles) that pull the leg toward the midline generate contractions that tear the connection between the tendon and the pubic bone. This often leads to inflammation and swelling that is perceived as pain in the area when examined and demonstrates specific findings of swelling, muscle separation and boney changes on MRI. The rectus muscle counterbalances the adductor muscles and they too can be torn and injured. This is usually the result of having stronger adductor muscles than rectus muscle. The treatment should first be rest and under the guidance of a physician or therapist NSAIDs may be used. Most individuals will require 3 months of reduced activity and rest.
Nerve Entrapment
In some circumstances, the aponeurosis (the outermost abdominal layer of the groin) of the external oblique can develop small fractures in the connective tissue. These small fractures are somewhat like the small openings in a pie crust. There are two nerves that lay just beneath this layer, the ilioinguinal and genital branch of the genital femoral nerve. Just beneath these nerves is a layer of connective tissue called the transversalis fascia. During certain movements and activities that lead to a rise in intra-abdominal pressure the nerves become sandwiched and squeezed between these two layers. Its theorized that the nerves or small branches off these nerves are pushed through the small openings of the external oblique creating a “pinching” effect and leading to pain.
Occult Hernia
The majority of sports hernias are the result of gradual weakening and failure of the transversalis fascia. This is the thin layer of connective tissue that makes up the back wall of the inguinal canal. In many ways it is similar to acquired groin hernias where a bulge can be felt. This weakening can often be appreciated on MRI.
Evaluation and Management
The evaluation and management of chronic groin pain and sports related groin injuries is challenging and should be performed by an expert in the field. There is no one way that all groin injuries are evaluated or managed. Some patients benefit from rest and a short course of anti-inflammatory medications, whereas, others require in depth radiologic evaluation, physical therapy and potentially surgery.
Dr Scott Laker has extensive experience with the management of sports hernias and is considered one of Michigan’s premier surgeons in the evaluation and management of chronic groin pain related to sports. He has helped many athletes return to their full activity and maintain their success on the court, field and ice.